
|
Groin strains or tendinopathies generally occur with sports such as martial arts, football or ice hockey. The muscle belly-tendon part of the adductor tendon or where this tendon inserts to the pubic (hip) bone is generally tender when pressure is placed on it. The adductor longus muscle is the most commonly injured. Common risk factors to increasing the risk of injury the groin muscles include a weakness in adductor muscles and a core muscle weakness (tranversus abdominals). The key differences between groin strains and tendinopathies are notably:
These injuries can respond very well to physiotherapy management which may include dry needling, manual therapy, extracorporeal shockwave, core stability, stretching and eccentric strengthening rehabilitation programs. Note for that groin related tendon injuries, exercise rehabilitation can take 3-6 weeks before full recovery can occur. 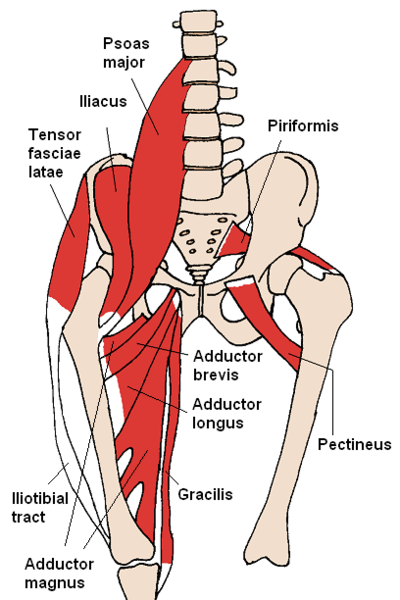
0 Comments
Plantar fasciitis or "inner heel pain" can be a very painful condition that is the result of degeneration of the plantar fascia origin on the inside of the heel bone as well as the surrounding soft tissue supporting structures. The plantar fascia has a key role in providing arch support and shock absorption during weight bearing activities such as standing, walking and running. It is often caused by an overuse or repetitive strain injury. Specifically, overuse causes micro-tears of the plantar fascia. Common risk factors include:
Before consider a cortisone injection, plantar fasciitis generally responds well to physiotherapy treatment including manual therapy, extracorporeal shockwave therapy, dry needling, stretches and specialised high load strengthening exercises. 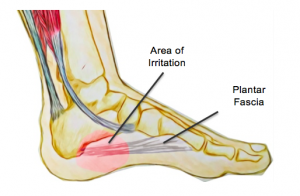 Subacromial pain syndrome is a non-traumatic one sided condition of the shoulder. This common condition is two thirds of all shoulder complaints at Acland Street Physiotherapy. This condition is more prevalent as you age. It usually causes pain localised around the acromion (bony process of the shoulder) when lifting the arm. Usually one or structures are injured within the subacromial space. Common conditions that cause subacromial pain syndrome include:
The above conditions often respond very well to physiotherapy treatment which includes manual therapy, dry needling, extracorporeal shockwave therapy, exercise programs involving stretching, strengthening the rotator cuff and stabilising the scapula (shoulder blades). 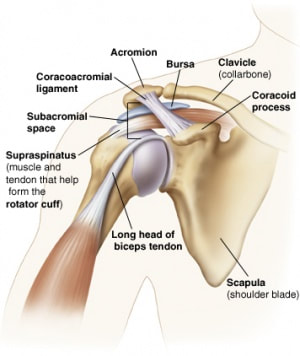 Tendons and ligaments have poor blood supply as they do not have direct blood vessels travelling through them. As a result of the poor blood supply, they are generally slow to heal. Shockwave Therapy has been clinically proven to naturally accelerate healing by targeting injured soft tissues with acoustic waves through:
Clinical Indications:
Contraindications:
When should you consider Shockwave Therapy? Shockwave Therapy is often considered as an alternative to surgery when traditional conservative management with a physiotherapist or podiatrist fails, as it is non-invasive, safe and can be highly effective for tendinopathies. Leading physiotherapists often combine traditional exercise rehabilitation and manual treatment with shockwave therapy to optimise outcomes. Are there any particular restrictions after treatment? You are generally advised to rest from physical activity for about 48 hours after each treatment session. What is the latest evidence for Shockwave Therapy? The best evidence for the use of Shockwave Therapy was available for tendon disorders and tendon calcifications in a “comprehensive rehabilitation framework.” (The Journal of Bone and Joint Surgery: February 7, 2018 - Volume 100 - Issue 3 - p 251–263) Randomised control trial for Achilles Tendinopathy: Eccentric loading alone was less effective when compared with a combination of eccentric loading and repetitive low-energy shock-wave treatment. (The American Journal of Sports Medicine 2017 Volume: 37 issue: 3, page(s): 463-470_ Systematic Review on Shockwave Therapy and Soft Tissue Injuries: There is evidence that Shockwave Therapy is effective for a number of soft tissue musculoskeletal conditions, particularly for plantar fasciitis, calcific tendinitis. There is a low level evidence for lack of benefit for non-calcific rotator cuff disease and mixed evidence in lateral epicondylitis. (British Journal of Sports Medicine 2014; 48 1521-1521) 3. How will you incorporate Shockwave Therapy into a physiotherapy consultation? As per normal routine, the patient will require a 40 minute initial consultation to conduct a comprehensive examination and require 20 minute follow up sessions. 3-5 weekly treatments may be required with shockwave therapy. A standard exercise rehabilitation as well as potentially other physiotherapy treatment techniques if clinically indicated. FREQUENTLY ASKED QUESTIONS 1. Does the treatment hurt? You will generally feel discomfort. Treatments last for about 5 minutes so they are generally tolerable. The dosage can also be adjusted by the physiotherapist to cater for comfort. However in general, the higher the dose, the more effective the treatment outcomes. 2. How many sessions will I need? 3-5 in general depending on the condition, its severity, patient tolerance and tissue response. Often, patients will feel immediate relief after the first session. 3. Will I feel pain after the treatment? You will often feel discomfort within 2 hours after the treatment. This is generally tolerable and not functionally limiting. |
Author
Archives
May 2024
|
 RSS Feed
RSS Feed